Discoid Meniscus: What to Look For?
- Randon Hall, MD

- Jul 19, 2019
- 2 min read
Updated: Mar 30, 2020

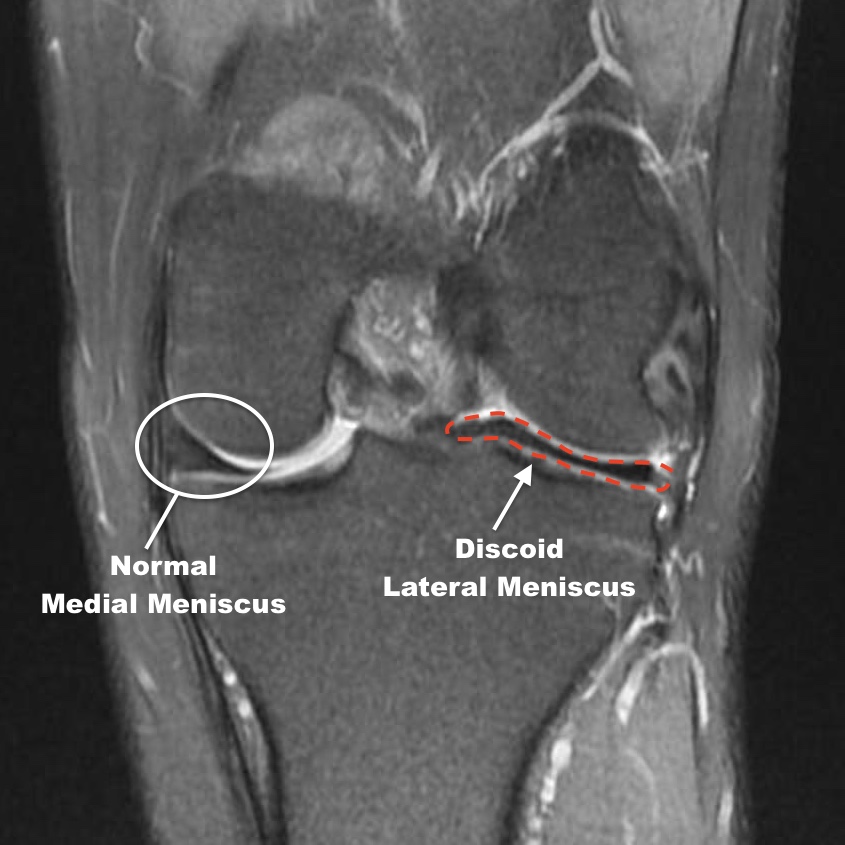
A discoid meniscus is essentially an abnormally shaped meniscus which can cause significant mechanical symptoms or be present with no symptoms at all. To fully understand why this happens, you need to take a deeper look at how the normal anatomy compares to the abnormal discoid meniscus. The normal meniscus is typically described as “C-shaped” which allows the femur to glide smoothly when the knee flexes and extends. However, when a discoid meniscus is present there is extra meniscal tissue creating more of a circular (discoid) shape. With a discoid meniscus, when the knee bends the abnormal tissue obstructs the proper flexion and extension of the knee.
Pop Goes the Knee
There are a few classic findings that may be apparent when encountering an athlete with a discoid meniscus. The first would be true mechanical symptoms where the patient has an audible and palpable popping sensation with flexing or extending the knee. I have experience with multiple discoid meniscus patients who presented with an extremely loud snapping sound and clunk of the knee (example below). Additionally, the athlete may not present until the discoid meniscus develops a tear, at which point they may have pain and swelling associated with the mechanical symptoms.
Advanced Imaging
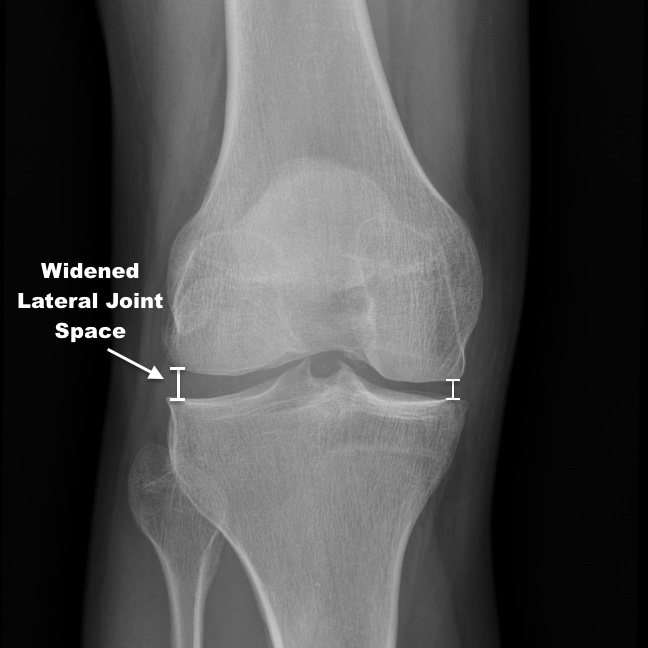
Generally, once the discoid meniscus is suspected, additional imaging can be ordered. If you start with a simple x-ray, look for a subtle finding of the lateral joint-line appearing wider than the medial side due to the presence of the discoid tissue. MRI can further be ordered to confirm the diagnosis.


When to Consider Surgery
If the discoid meniscus is asymptomatic (no pain or disability) or is otherwise found incidentally on an MRI then simply observing over time would be appropriate. As you would expect, a discoid meniscus is much more susceptible to tearing than the normal meniscus. If the patient is having pain, swelling, reduced ROM or a tear is seen on MRI then surgical treatment may be necessary. The procedure is called a saucerization, which is a reshaping of the meniscus in order to maintain as much tissue as possible while correcting the mechanical block. Typically patients do well with the procedure and return to full sports.
Photos:
1. Case courtesy of Dr Heather Pascoe, Radiopaedia.org, rID: 58282 (modified)
2. Case courtesy of Dr Hani Salam, Radiopaedia.org, rID: 35594 (modified)



Comments